


Common Nerve Compression Symptoms & Causes
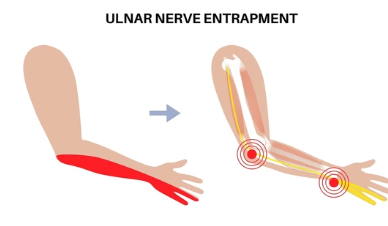
Nerve compression symptoms include deep aching pain often described as burning or electric, weakness affecting specific muscle groups, muscle atrophy developing with chronic compression, numbness or tingling in nerve distribution, symptoms worsening with certain positions, night pain disturbing sleep, and progressive functional limitations. Suprascapular nerve compression causes posterior shoulder pain, weakness with overhead activities and external rotation, and visible supraspinatus and infraspinatus atrophy. Axillary nerve compression presents with lateral shoulder pain, deltoid weakness, and numbness over lateral shoulder. Long thoracic nerve injury causes scapular winging and difficulty elevating the arm. Thoracic outlet syndrome causes neck and shoulder pain radiating down arm, hand numbness particularly ulnar distribution, arm fatigue, and symptoms worsening overhead. Carpal tunnel syndrome causes hand numbness in thumb through middle finger and night symptoms. Cubital tunnel syndrome causes numbness in ring and small fingers.
Causes include ganglion cysts arising from joint pathology compressing nearby nerves; repetitive activities in athletes and workers creating traction neuropathy; trauma including fractures and dislocations directly injuring nerves; anatomic variations such as narrow passages or cervical ribs; post-surgical complications from scarring or hardware; sleeping positions with prolonged compression; tumors compressing nerves; inflammatory conditions including brachial neuritis; diabetes predisposing to compression; and prolonged pressure from casts or positioning.
Schedule Your ConsultationWho's at risk for Nerve Compressions?
Several factors increase risk of nerve compressions. Understanding risk factors enables prevention strategies:
Athletes and Repetitive Workers
+Athletes performing repetitive overhead motions face highest risk. Volleyball players develop suprascapular nerve traction from repetitive serving. Baseball pitchers experience nerve stretch during throwing. Swimmers performing high-volume training stress nerves repetitively. Tennis players, weightlifters, and cyclists face specific risks. Occupational groups including painters, electricians, construction workers, computer workers, assembly workers, and musicians performing prolonged repetitive movements develop compression. Weekend warriors suddenly increasing activity risk acute injuries.
Anatomic and Postural Factors
+Anatomic variations significantly affect compression risk. Narrow passages with tight ligaments predispose to entrapment including narrow suprascapular notch, tight carpal tunnel, and narrow cubital tunnel. Cervical ribs and anomalous ribs cause thoracic outlet syndrome. Tight muscles compress nerves. Poor posture with rounded shoulders narrows spaces. Hypermobility creates repetitive traction. Bone spurs and arthritis narrow passages.
Medical Conditions
+Diabetes dramatically increases compression susceptibility through metabolic changes. Hypothyroidism, rheumatoid arthritis, pregnancy with fluid retention, obesity, and kidney disease increase risk. Previous nerve injuries create vulnerability. Smoking impairs nerve healing. Excessive alcohol causes nutritional deficiencies. Vitamin deficiencies particularly B vitamins compromise nerve health. Rapid weight loss decreases protective padding.
Trauma and Surgery
+Fractures risk direct nerve injury or compression from callus and hardware. Dislocations can stretch or contuse nerves. Previous surgeries risk nerve injury from retraction, hardware compression, or scarring. Heavy backpack use, sleeping with arms compressed, and prolonged positioning risk compression. Repetitive movements in specific occupations create cumulative trauma.
Nerve Compression Prevention

Prevention focuses on reducing nerve stress and addressing risk factors. For athletes and workers, implement proper training avoiding excessive volume, adequate rest periods, graduated return after layoffs, strengthening programs, and technique optimization. Cross-training reduces repetitive stress. Use proper ergonomics with neutral positions, frequent breaks, proper tool design, and ergonomic assessments. Computer workers should maintain neutral wrist position.
Correct postural abnormalities through strengthening, stretching, and maintaining neutral positions. Maintain healthy weight. Control diabetes, thyroid disorders, and other medical conditions through management. Ensure adequate nutrition including B vitamins. Avoid smoking and excessive alcohol. Minimize backpack weight. Sleep positions should avoid prolonged compression of elbows bent, wrists flexed, or arms overhead.
For those with anatomic risk factors, activity modifications and monitoring identify early symptoms. Recognize warning signs including persistent pain, weakness, numbness, or atrophy warranting prompt evaluation. Address underlying joint instability creating secondary compression. Once significant compression with atrophy exists, prevention is no longer possible. Early intervention when symptoms are mild offers dramatically better outcomes than waiting.
How are Nerve Compressions Diagnosed?
Diagnosis begins with detailed history documenting pain quality and location, weakness patterns, numbness distribution, symptom onset, aggravating activities, previous injuries or surgeries, occupational demands, medical conditions including diabetes, and muscle wasting. Physical examination includes inspection for visible atrophy comparing sides, palpation over nerve pathways for tenderness or masses, strength testing isolating specific muscles, range of motion assessment, and provocative maneuvers reproducing symptoms. Sensory testing maps numbness patterns following nerve distributions.
Electrodiagnostic testing is critical for diagnosis. Electromyography shows denervation potentials in affected muscles, documents distribution matching nerve territories, distinguishes nerve compression from other pathology, and assesses chronicity and severity. Nerve conduction studies measure signal transmission, identify conduction block at compression sites, and assess prognosis. Testing should be performed at least 3-4 weeks after onset. MRI with specialized sequences directly visualizes nerves, identifies structural causes including ganglion cysts appearing as bright fluid masses, evaluates muscle atrophy and fatty infiltration, and shows associated pathology. Ultrasound identifies superficial nerve pathology and guides injections. CT evaluates bony abnormalities including cervical ribs and bone spurs. Diagnostic nerve blocks can confirm diagnosis when symptoms temporarily resolve.
What treatment is best for Nerve Compressions?
Treatment depends on compression cause, severity and duration, degree of atrophy, and symptoms. Early intervention before irreversible damage offers best outcomes. Many compressions respond to conservative treatment while others require surgery. Treatment is individualized based on comprehensive evaluation.
Conservative Management
+Initial treatment focuses on activity modification avoiding provocative positions and repetitive activities. Splinting maintains optimal positions including wrist splints for carpal tunnel and elbow pads for cubital tunnel. Physical therapy emphasizes nerve gliding exercises, strengthening, postural correction, and ergonomic education. NSAIDs reduce inflammation. Corticosteroid injections decrease inflammation and provide diagnostic information. Medical management of underlying conditions including diabetes control and thyroid replacement. Conservative treatment is most effective when started early, typically within 3-6 months. Electrodiagnostic testing monitors recovery. Continued weakness, progressive atrophy, or symptoms beyond 3-6 months despite treatment warrant surgical consideration.
Surgical Nerve Decompression
+Nerve compressions from structural causes or failing conservative treatment require surgical decompression. Suprascapular nerve decompression involves excising ganglion cysts, releasing tight ligaments, and repairing joint pathology. Carpal tunnel release divides transverse carpal ligament through open or endoscopic approach. Cubital tunnel surgery involves in situ decompression or ulnar nerve transposition. Thoracic outlet decompression includes first rib resection or scalenectomy. Surgery relieves pain rapidly but strength recovery depends on preoperative atrophy. Mild atrophy may fully recover in 6-12 months while severe chronic atrophy shows limited improvement. Early surgery before significant atrophy optimizes recovery.
Minimally Invasive Techniques
+Many decompressions can be performed minimally invasively offering smaller incisions, less trauma, faster recovery, and reduced scarring. Endoscopic carpal tunnel release uses small incisions and camera guidance. Arthroscopic suprascapular nerve decompression visualizes compression through small portals. Ultrasound-guided techniques assist localization. Minimally invasive approaches reduce post-operative pain and allow earlier return while achieving same decompression. Not all compressions are amenable to endoscopic treatment. Complex cases, revisions, or those requiring extensive dissection may require open approach.
Nerve Reconstruction
+Severe injuries with complete disruption or prolonged denervation causing irreversible atrophy may require reconstruction. Nerve grafting bridges gaps using donor segments. Nerve transfer procedures reroute expendable nerves to reinnervate critical muscles when proximal recovery impossible. Tendon transfers provide function when nerve recovery not feasible. These reconstructions are reserved for severe cases. Early consultation optimizes outcome as delay beyond 12-18 months reduces recovery potential. Neurolysis removes scar tissue entrapping nerves.
Nerve Compression Treatment in Cleveland, Ohio

Cleveland Shoulder Institute specializes in comprehensive evaluation and treatment of peripheral nerve compressions. Our fellowship-trained specialists have extensive experience managing complex nerve entrapments throughout the upper extremity.
We offer complete assessment including detailed physical examination, coordination with neurologists for comprehensive electrodiagnostic testing, high-resolution MRI with specialized nerve sequences, and ultrasound visualization. Conservative treatment includes specialized physical therapy with nerve gliding, strengthening, posture correction, and ergonomic modifications. We offer image-guided injections when indicated. For cases requiring surgery, we perform advanced decompression throughout the upper extremity including arthroscopic and open suprascapular nerve release, carpal tunnel release, cubital tunnel decompression, thoracic outlet decompression, and other specific releases. We have expertise in minimally invasive techniques and complex reconstruction. Our approach emphasizes precise anatomic decompression while protecting structures. Post-operative rehabilitation follows evidence-based protocols optimizing recovery. Located in Cleveland with comprehensive resources for complex nerve problems.
Schedule Your ConsultationMeet our Nerve Compression Team
Dr. Gobezie is a fellowship-trained orthopedic surgeon with specialized expertise in peripheral nerve problems. He has advanced training in nerve compression syndromes, decompression techniques, and reconstruction procedures. Dr. Gobezie collaborates closely with neurologists and electrophysiologists ensuring accurate diagnosis. He maintains expertise through active participation in nerve research, teaching commitments, and attendance at specialized conferences.
Supporting Dr. Gobezie are fellowship-trained neurologists performing electrodiagnostic testing, board-certified anesthesiologists, skilled surgical teams, specialized physical therapists understanding nerve rehabilitation, occupational therapists providing ergonomic guidance, and dedicated medical staff. This collaborative approach ensures accurate localization through clinical and electrodiagnostic correlation, identification of structural causes, appropriate treatment selection, expert surgical technique, structured rehabilitation supporting recovery, ergonomic modifications preventing recurrence, and long-term monitoring. Our team understands nerve compressions significantly impact quality of life, providing expert care focused on relieving pain, restoring strength, and optimizing recovery.
What Our Patients Say About Nerve Compression Treatment
Real experiences from patients who successfully treated nerve compressions:
"I had severe weakness as a volleyball player that no one could figure out. Dr. Gobezie diagnosed suprascapular nerve compression from a cyst. After arthroscopic surgery my pain resolved immediately and my strength gradually returned. Eighteen months later I am back playing competitively. His expertise saved my athletic career."
— Jessica Rodriguez
"Numbness in my hand from carpal tunnel was affecting my work as a programmer. Dr. Gobezie performed endoscopic carpal tunnel release and the recovery was quick. Symptoms improved within days and I was back typing within two weeks. The minimally invasive approach made a huge difference in recovery time."
— David Kumar
"I struggled with numbness and arm fatigue from thoracic outlet syndrome for years. Dr. Gobezie clearly explained the anatomy and treatment options. After first rib resection surgery and physical therapy, my symptoms are 90% better. His surgical skill and comprehensive approach made all the difference. Highly recommend for nerve compression issues."
— Amanda Foster
Nerve Compression Frequently Asked Questions
How long does it take for nerve compression symptoms to improve with treatment?
+Recovery timeline depends on compression severity and duration. With conservative treatment for mild compression, pain may improve within weeks but strength recovery takes 2-6 months as nerve healing occurs slowly. After surgical decompression, pain typically improves rapidly within days to weeks. Muscle strength and atrophy recovery is slower—mild atrophy may recover in 6-12 months while moderate atrophy requires 12-18 months. Severe chronic atrophy present over 18-24 months may never fully recover as muscle changes become irreversible. Early treatment before significant atrophy develops offers best recovery potential. Nerve regeneration occurs at approximately 1 inch per month.
Can nerve compression cause permanent damage?
+Yes, prolonged nerve compression can cause irreversible damage. Initially, compression causes temporary nerve dysfunction that fully recovers once pressure is relieved. However, chronic compression leads to progressive nerve fiber degeneration and muscle atrophy. After approximately 12-18 months of denervation, muscle undergoes fatty infiltration and fibrosis making recovery impossible even with successful nerve decompression. This is why early diagnosis and treatment is critical. Mild symptoms should not be ignored—progressive weakness or visible muscle wasting warrant urgent evaluation. Early surgical decompression before irreversible changes occur offers excellent recovery potential.
What is the difference between nerve compression and tendon tears?
+Both cause weakness but have different mechanisms and treatments. Tendon tears cause mechanical weakness from structural disruption—muscles can generate force but cannot transmit it effectively to bone. Nerve compression causes neurologic weakness from denervation—muscles cannot generate force even though tendons are intact. EMG testing is critical for differentiation showing denervation patterns in nerve compression but normal electrical activity in tendon tears. MRI shows both conditions. Some patients have both complicating diagnosis. Accurate differentiation is essential as treatments differ—tendon tears need repair while nerve compression requires decompression.
Will I need surgery for nerve compression?
+Not necessarily. Many nerve compressions respond to conservative treatment including activity modification, splinting, physical therapy, and anti-inflammatory measures, particularly when identified early without significant muscle atrophy. Surgery is recommended when structural causes like ganglion cysts or bone spurs compress nerves, conservative treatment fails after appropriate trial (typically 3-6 months), progressive muscle atrophy develops despite treatment, significant functional limitations persist, or vascular compromise threatens limb viability. Your surgeon evaluates compression severity, underlying cause, symptom duration, and EMG findings determining optimal treatment. Early mild compression may resolve without surgery while advanced cases require decompression.
Can nerve compression return after treatment?
+Recurrence is uncommon with appropriate treatment. After surgical decompression, recurrence rate is typically under 10% usually from scar tissue formation, incomplete initial decompression, or development of new pathology. Carpal tunnel syndrome has recurrence rates of 5-10%. Preventive measures include completing full rehabilitation program, maintaining proper ergonomics and body mechanics, avoiding provocative activities until fully healed, controlling medical conditions like diabetes, and gradual return to activities with proper technique. Regular follow-up examinations monitor for early signs of recurrence. If symptoms return, prompt evaluation determines cause and guides additional treatment.