

Common AC Separation Symptoms & Causes

AC separation symptoms include immediate pain at the top of the shoulder following injury, visible bump or step-off deformity where the clavicle elevates (more prominent in higher grades), swelling and bruising over the AC joint, pain worsened by arm movement particularly reaching across the body, difficulty sleeping on the affected side, weakness with overhead activities and lifting, and tenderness directly over the AC joint. Higher grade separations show obvious deformity with the clavicle prominently elevated creating a visible step-off compared to the opposite shoulder.
Causes are almost exclusively traumatic. Falls directly onto the point of the shoulder are most common, frequently occurring in cycling crashes, football tackles, hockey checks, skiing falls, and motorcycle accidents. Direct blows to the top of the shoulder during contact sports cause similar injury. The force drives the acromion downward while the clavicle remains in position, tearing the connecting ligaments. Less commonly, falls onto an outstretched hand transmit force upward causing separation. The mechanism and force magnitude determine injury severity.
Schedule Your ConsultationWho's at risk for AC Separation?
Several factors increase AC separation risk. Understanding these helps with prevention:
Contact Sports Athletes
+Football players, particularly those in tackling positions, face high AC separation rates from direct shoulder contact. Hockey players sustain separations from checks into boards. Rugby, lacrosse, and wrestling athletes experience similar mechanisms. These sports involve frequent falls and direct shoulder trauma.
Cyclists and Motorcyclists
+Cycling crashes commonly cause AC separations when riders fall directly onto the shoulder. Road cyclists, mountain bikers, and motorcycle riders are particularly vulnerable. The combination of speed and hard landing surfaces creates significant force transmission to the AC joint.
Winter Sports
+Skiers and snowboarders sustain AC separations from falls onto hard snow or ice. The shoulder often absorbs impact during falls at speed. Ice hockey combines contact sport mechanisms with hard ice surface falls increasing risk.
Previous AC Joint Injury
+Those with previous AC joint sprains or separations may have residual ligament weakness predisposing to reinjury with less force. Incomplete healing or inadequate rehabilitation following prior injury increases vulnerability. Some individuals have inherently looser ligaments increasing separation susceptibility.
AC Separation Prevention

Prevention focuses on reducing fall risk and using appropriate protective equipment. Athletes in contact sports should use properly fitted shoulder pads that adequately protect the AC joint. Football players, hockey players, and lacrosse players benefit from equipment designed to absorb and distribute impact forces. Proper tackling and checking technique reduces direct shoulder impact.
Cyclists should wear appropriate protective gear and develop skills to fall safely when possible—rolling rather than absorbing impact on the shoulder point. Maintain bicycle in good condition to prevent mechanical failures causing crashes. Mountain bikers should ride within skill level and use appropriate protective equipment. Skiers and snowboarders should progress gradually to challenging terrain and consider impact protection. Strengthen shoulder muscles including deltoid, trapezius, and rotator cuff to provide some dynamic protection. Once AC separation occurs, prevention is no longer possible—focus shifts to appropriate treatment based on injury grade.
How is AC Separation Diagnosed?
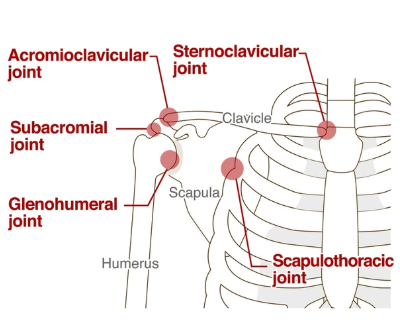
Diagnosis begins with history documenting injury mechanism (typically direct fall onto shoulder), immediate symptoms, and functional limitations. Physical examination reveals tenderness directly over the AC joint, visible step-off deformity in higher grade injuries, pain with cross-body adduction (reaching across to opposite shoulder), and positive piano key sign where the elevated clavicle can be pushed down then springs back up.
X-rays are essential for diagnosis and grading. Standard views show widening of the AC joint space and elevation of the clavicle relative to the acromion. Stress views with the patient holding weights may accentuate displacement in subtle cases. Comparison views of the opposite shoulder help quantify displacement. The Rockwood classification grades injury severity: Type I shows normal X-rays with ligament sprain, Type II shows slight clavicle elevation, Type III shows 25-100% clavicle elevation, Types IV-VI show severe displacement in various directions. MRI is rarely needed but can evaluate associated injuries including rotator cuff tears in complex cases. Accurate grading guides treatment decisions.
What treatment is best for AC Separation?
Treatment depends primarily on injury grade. Low-grade separations (Types I-II) are treated conservatively with excellent outcomes. High-grade separations (Types IV-VI) typically require surgery. Type III injuries are controversial with treatment individualized based on patient factors.
Conservative Management
+Type I and II separations heal well without surgery. Treatment includes sling immobilization for comfort (typically 1-2 weeks), ice and anti-inflammatory medications for pain, early range of motion as tolerated, progressive strengthening once pain subsides, and return to activities in 2-6 weeks depending on severity. The ligaments heal with some residual laxity but patients achieve full function. Some visible bump may persist but is rarely problematic.
Type III Injury Management
+Type III separations remain controversial. Many heal well with conservative treatment similar to lower grades. However, some patients—particularly young athletes, overhead workers, and those with heavy physical demands—may benefit from surgical reconstruction. Initial conservative trial is often recommended with surgery considered if symptoms persist or function remains limited at 3-6 months. Individualized decision-making considers activity level, occupation, and patient preferences.
Acute Surgical Reconstruction
+Types IV-VI separations and selected Type III injuries benefit from surgical reconstruction. Acute repair within 2-3 weeks offers best outcomes before ligaments retract and scar. Techniques include coracoclavicular ligament repair or reconstruction using suture anchors, suture buttons, or tendon grafts. The goal is anatomic reduction of the clavicle and restoration of ligament stability. Modern techniques achieve excellent outcomes with 85-90% good to excellent results.
Chronic Reconstruction
+Patients with chronic symptomatic AC separations—those presenting months after injury or with failed conservative treatment—may require reconstruction using tendon graft. The coracoclavicular ligaments are reconstructed using autograft or allograft tissue creating new ligament connections. Distal clavicle excision may be added to address AC joint arthritis. Outcomes are good though slightly less predictable than acute repairs.
AC Separation Treatment in Cleveland, Ohio

Cleveland Shoulder Institute specializes in comprehensive evaluation and treatment of all AC separation grades. Our fellowship-trained shoulder surgeons have extensive experience with both conservative management and surgical reconstruction techniques including modern anatomic coracoclavicular reconstruction.
We provide thorough diagnostic evaluation including physical examination, appropriate X-ray imaging with stress views when indicated, and accurate injury classification guiding treatment decisions. Conservative management includes structured rehabilitation protocols with experienced physical therapists. For injuries requiring surgery, we utilize current reconstruction techniques with proven outcomes. Our approach emphasizes individualized treatment based on injury severity, patient activity level, and functional demands. Located in Cleveland with urgent evaluation available for acute injuries.
Schedule Your ConsultationMeet our AC Separation Team
Dr. Gobezie is a fellowship-trained shoulder and elbow surgeon with extensive experience treating all grades of AC separations. He has expertise in both conservative management protocols and surgical reconstruction techniques including anatomic coracoclavicular ligament reconstruction. His approach emphasizes accurate diagnosis, appropriate treatment selection, and individualized care.
Supporting Dr. Gobezie are board-certified anesthesiologists, experienced surgical teams, specialized physical therapists understanding AC joint rehabilitation protocols, and dedicated medical staff. This collaborative approach ensures accurate injury classification, optimal treatment selection, expert surgical technique when indicated, and structured rehabilitation for best outcomes.
What Our Patients Say About AC Separation Treatment
Real experiences from patients who successfully treated AC separations:
"I separated my AC joint in a cycling crash. Dr. Gobezie accurately graded my Type II injury and recommended conservative treatment. Six weeks of therapy and I was back riding with full strength. The bump is barely visible now. Great outcome without surgery."
— Brian Mitchell
"My severe AC separation from a football injury needed surgical reconstruction. Dr. Gobezie repaired the ligaments within two weeks of injury. Recovery took time but my shoulder is completely stable now with no deformity. Excellent surgical result."
— Marcus Thompson
"After months of pain from an old AC separation, I finally had reconstruction surgery. Dr. Gobezie used a tendon graft to rebuild my ligaments. The chronic pain is gone and I can lift overhead without problems. Worth the recovery time."
— Kevin Roberts
AC Separation Frequently Asked Questions
Will the bump on my shoulder go away?
+For Type I injuries, the bump typically resolves completely. Type II and III separations often leave some permanent visible prominence where the clavicle remains slightly elevated. This is usually painless and cosmetic only. Surgical reconstruction can reduce the deformity but some residual prominence may remain. Most patients tolerate the cosmetic change well given full functional recovery.
Do all AC separations need surgery?
+No. Type I and II separations heal well with conservative treatment—sling, ice, therapy. Type III injuries are controversial with many healing conservatively though some benefit from surgery. Types IV-VI typically require surgical reconstruction. Your surgeon evaluates injury grade, activity level, and functional demands to recommend optimal treatment. Most AC separations are successfully treated without surgery.
How long is recovery from AC separation?
+Conservative treatment for Type I-II injuries allows return to activities in 2-6 weeks. Type III injuries treated conservatively may require 6-12 weeks. Surgical reconstruction requires sling immobilization for 6 weeks, therapy for 3-4 months, and return to contact sports at 4-6 months. Full recovery and strength restoration may take 6-9 months after surgery.
Can I return to contact sports after AC separation?
+Yes, most athletes successfully return to contact sports after AC separation treatment. Conservative treatment for low-grade injuries allows return in weeks. Surgical reconstruction requires longer recovery but achieves stable results allowing full contact participation. Protective padding over the AC joint during initial return reduces reinjury risk. Your surgeon guides sport-specific return timing.
What happens if AC separation is left untreated?
+Low-grade separations typically heal well even without formal treatment though rehabilitation optimizes outcomes. High-grade separations left untreated may result in chronic pain, weakness with overhead activities, visible deformity, and accelerated AC joint arthritis. Delayed treatment is possible but outcomes are somewhat less predictable than acute management. Seek evaluation for accurate grading and treatment recommendations.