

Common Labral Tear Symptoms & Causes

Labral tear symptoms include deep shoulder pain often difficult to localize, mechanical symptoms such as catching, clicking, or popping during movement, sensation of instability or shoulder "giving way," pain with overhead activities particularly throwing, night pain especially when sleeping on the affected side, decreased range of motion, weakness during specific movements, and pain reaching behind the back. SLAP tears typically cause pain at the top of the shoulder worsened by overhead activities and may affect throwing velocity and control. Bankart tears cause instability with apprehension during certain arm positions and may result in recurrent dislocations or subluxations.
Causes include traumatic shoulder dislocation—the most common cause of Bankart lesions, with over 90% of anterior dislocations causing labral damage; falls onto an outstretched arm compressing the shoulder; repetitive overhead activities in baseball pitchers, swimmers, volleyball players, and tennis players causing SLAP tears from microtrauma; direct trauma to the shoulder; heavy lifting particularly with arms extended; motor vehicle accidents; and age-related degeneration with labral fraying developing gradually over time.
Schedule Your ConsultationWho's at risk for Labral Tears?
Several factors increase your risk of developing labral tears. Understanding these helps with prevention and early detection:
Overhead Athletes
+Athletes performing repetitive overhead motions face highest risk for SLAP tears. Baseball pitchers experience tremendous forces on the labrum during throwing. Swimmers, volleyball players, tennis players, and quarterbacks develop tears from cumulative microtrauma. Poor technique, excessive training volume, and inadequate rest accelerate development.
Previous Shoulder Dislocation
+Shoulder dislocations cause labral tears in over 90% of cases. Younger patients under 25 who dislocate face 70-90% risk of recurrent instability without surgical repair. Each subsequent dislocation causes additional labral and bone damage. Those with one dislocation are at high risk for labral pathology.
Contact Sports and Trauma
+Athletes in contact sports including football, hockey, rugby, and wrestling face elevated risk from direct trauma and falls. Motor vehicle accidents, bicycle crashes, and falls onto outstretched arms cause acute labral tears. High-energy trauma may cause complex tears involving multiple labral regions.
Age and Degeneration
+Labral tissue degenerates with age, becoming more susceptible to tearing with minor trauma. Degenerative SLAP tears are common in patients over 40. These often respond to conservative treatment or biceps tenodesis rather than repair. Underlying shoulder laxity or hypermobility increases tear susceptibility.
Labral Tear Prevention

Prevention focuses on maintaining shoulder stability and avoiding excessive stress. For overhead athletes, implement proper training programs with adequate rest between sessions, pitch count limitations for baseball players, proper throwing mechanics with qualified coaching, and graduated return after layoffs. Strengthen rotator cuff and scapular stabilizers supporting shoulder mechanics. Address any shoulder pain promptly before minor issues progress.
For those who have experienced shoulder dislocation, discuss surgical stabilization with your surgeon—young active patients benefit from early repair preventing recurrent instability and progressive labral damage. Use proper technique when lifting heavy objects, keeping weight close to the body and avoiding extreme arm positions. Maintain overall shoulder conditioning through balanced strengthening and flexibility exercises. Wear appropriate protective equipment in contact sports. Once significant labral tear occurs, prevention is no longer possible—focus shifts to appropriate treatment preventing further damage and restoring function.
How are Labral Tears Diagnosed?
Diagnosis begins with detailed history documenting injury mechanism, symptom onset and progression, instability episodes including dislocations or subluxations, pain location and quality, mechanical symptoms, sport or activity demands, and previous shoulder injuries. Physical examination includes inspection for muscle atrophy, range of motion assessment, strength testing, and specific provocative tests. The O'Brien test and crank test evaluate SLAP tears. Apprehension and relocation tests assess anterior instability from Bankart lesions. Load and shift testing evaluates overall laxity.
Standard X-rays evaluate bone structure and identify bony Bankart lesions (bone loss from glenoid) or Hill-Sachs lesions (humeral head compression fractures from dislocation). MRI arthrography with intra-articular contrast is gold standard for labral evaluation, showing tear location, extent, and associated pathology including rotator cuff tears, biceps pathology, and cartilage damage. Standard MRI may miss subtle tears. CT scan with 3D reconstruction evaluates bone loss critical for surgical planning in instability cases. Diagnostic arthroscopy provides definitive diagnosis while allowing simultaneous treatment.
What treatment is best for Labral Tears?
Treatment depends on tear type and location, patient age and activity level, presence of instability, and functional goals. Not all labral tears require surgery—treatment is individualized based on comprehensive evaluation.
Conservative Management
+Many labral tears, particularly degenerative tears in older patients, respond to conservative treatment. Physical therapy emphasizes rotator cuff and scapular stabilizer strengthening, proprioceptive training, and activity modification. NSAIDs manage pain and inflammation. Corticosteroid injections provide temporary relief. Athletes may require activity modification or position changes. Conservative treatment is first-line for stable shoulders without recurrent instability.
Arthroscopic Labral Repair
+Surgical repair is indicated for tears causing instability, failed conservative treatment, or significant symptoms in active patients. Arthroscopic technique uses small incisions and suture anchors to reattach torn labrum to glenoid rim. Bankart repair addresses anterior-inferior tears restoring stability. SLAP repair reattaches the superior labrum and biceps anchor. Success rates exceed 85-90% for appropriately selected patients.
Biceps Tenodesis for SLAP Tears
+For SLAP tears in patients over 35-40 or those with degenerative tears, biceps tenodesis often outperforms labral repair. The biceps tendon is cut from its labral attachment and secured to the humerus, eliminating the pain source while preserving biceps function. This avoids risks of SLAP repair failure and provides more predictable outcomes in appropriate candidates.
Bone Loss Procedures
+Significant glenoid bone loss from recurrent dislocations may require bone augmentation procedures. Latarjet procedure transfers the coracoid process with attached muscle to the front of the glenoid, restoring bone stock and providing dynamic stability. This is indicated when glenoid bone loss exceeds 20-25% where soft tissue repair alone has high failure rates.
Labral Tear Treatment in Cleveland, Ohio

Cleveland Shoulder Institute specializes in comprehensive evaluation and treatment of all labral pathology. Our fellowship-trained shoulder surgeons have extensive experience with arthroscopic labral repair, SLAP repair and biceps tenodesis, Bankart repair for instability, and complex reconstruction including Latarjet procedure for bone loss.
We provide thorough diagnostic evaluation including physical examination with specific provocative testing, MRI arthrography for detailed labral assessment, and CT imaging for bone loss quantification when indicated. Treatment plans are individualized based on tear characteristics, instability pattern, patient age, and activity goals. Conservative management includes specialized physical therapy programs. Surgical treatment utilizes advanced arthroscopic techniques with proven outcomes. Located in Cleveland with comprehensive resources for complex labral pathology.
Schedule Your ConsultationMeet our Labral Tear Team
Dr. Gobezie is a fellowship-trained shoulder and elbow surgeon with specialized expertise in labral pathology and shoulder instability. He has extensive experience with arthroscopic labral repair, SLAP lesion treatment, and complex instability reconstruction including Latarjet procedure. His approach emphasizes accurate diagnosis, appropriate patient selection, and expert surgical technique.
Supporting Dr. Gobezie are board-certified anesthesiologists, experienced surgical teams trained in arthroscopic procedures, specialized physical therapists understanding post-repair rehabilitation protocols, and dedicated medical staff. This collaborative approach ensures accurate diagnosis, optimal treatment selection, expert surgical technique when indicated, and structured rehabilitation maximizing outcomes.
What Our Patients Say About Labral Tear Treatment
Real experiences from patients who successfully treated labral tears:
"After multiple shoulder dislocations playing football, Dr. Gobezie performed Bankart repair. My shoulder is completely stable now—no more instability or apprehension. The arthroscopic approach meant quick recovery. Back to full contact sports within six months."
— Marcus Johnson
"A SLAP tear was ending my pitching career. Dr. Gobezie recommended biceps tenodesis given my age and tear pattern. Best decision—pain is gone, I have full strength, and I am pitching competitively again. His expertise with overhead athletes showed."
— Daniel Rivera
"My labral tear caused constant clicking and pain. Physical therapy helped initially but symptoms returned. Arthroscopic repair fixed the problem permanently. Dr. Gobezie explained everything clearly and results exceeded expectations."
— Sarah Collins
Labral Tear Frequently Asked Questions
Can labral tears heal without surgery?
+Some labral tears improve with conservative treatment including physical therapy and activity modification. Degenerative tears in older patients often respond to non-surgical management. However, tears causing shoulder instability, recurrent dislocations, or significant symptoms in active patients typically require surgical repair for lasting improvement. Your surgeon evaluates tear characteristics and symptoms determining optimal treatment.
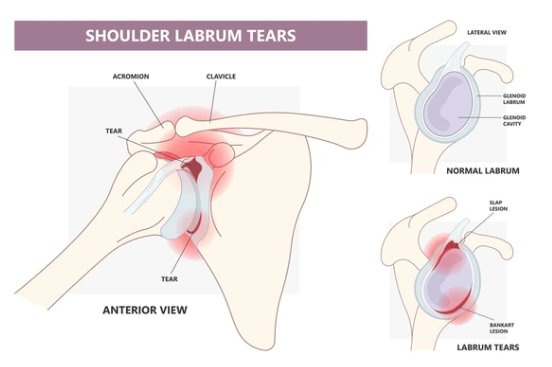
What is the difference between SLAP tear and Bankart lesion?
+SLAP tears affect the superior (top) labrum where the biceps tendon attaches, typically occurring in overhead athletes from repetitive throwing or falls. Bankart lesions involve the anterior-inferior (front-bottom) labrum, usually from shoulder dislocations causing instability. Treatment differs—SLAP tears may be repaired or treated with biceps tenodesis while Bankart lesions require repair to restore stability.
How long is recovery after labral repair?
+Recovery typically requires 4-6 months. The shoulder is immobilized in a sling for 4-6 weeks protecting the repair. Passive motion begins early, progressing to active motion around 6 weeks. Strengthening starts at 8-12 weeks. Return to overhead sports requires 4-6 months. Full recovery with complete strength restoration may take 6-9 months for throwing athletes.
Will I regain full shoulder function after surgery?
+Most patients regain excellent function after labral repair. Success rates exceed 85-90% for appropriate surgical candidates. Overhead athletes may experience slight changes in motion but typically return to pre-injury performance levels. Instability repairs provide stable shoulders allowing return to contact sports. Your surgeon discusses realistic expectations based on your specific tear and goals.
What happens if a labral tear is left untreated?
+Untreated labral tears causing instability lead to recurrent dislocations, progressive bone loss, cartilage damage, and eventual arthritis. Each dislocation causes additional damage making future repair more complex. SLAP tears may progress causing biceps pathology and ongoing pain. Early treatment prevents these complications and provides better long-term outcomes.