

Common Shoulder Impingement Symptoms & Causes
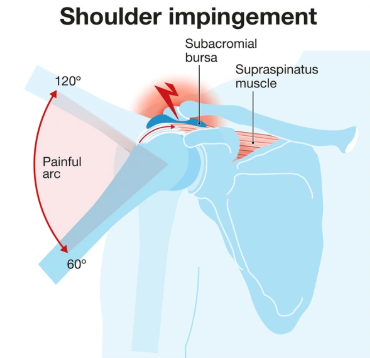
Primary symptoms include pain with overhead activities, difficulty reaching behind the back, weakness during lifting or throwing motions, night pain when sleeping on the affected shoulder, and painful arc between 60-120 degrees of arm elevation. Pain typically develops gradually over weeks to months, worsening with continued activity. Advanced cases show weakness from rotator cuff damage and catching sensations during movement.
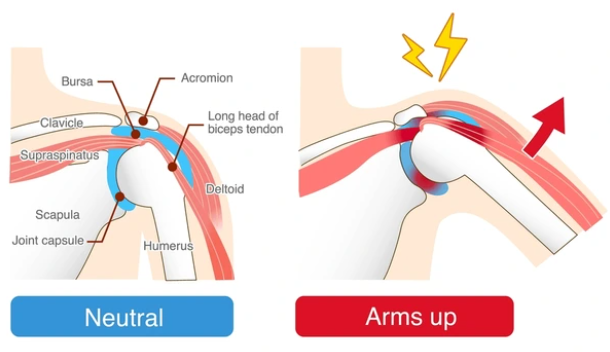
Causes include repetitive overhead activities in occupations like painting, construction, or hair styling; sports involving throwing, swimming, or overhead motions; anatomic factors including bone spurs, hooked acromion shape, or thickened ligaments; poor posture with rounded shoulders; rotator cuff weakness failing to stabilize the humeral head; scapular dyskinesis causing abnormal shoulder blade movement; and previous shoulder injuries creating altered mechanics.
Schedule Your ConsultationWho's at risk for developing Shoulder Impingement?
Several factors increase your risk of developing shoulder impingement. Understanding these risk factors helps with early detection and preventive strategies:
Age and Occupation
+Impingement most commonly affects people over 40 as age-related changes narrow the subacromial space. Occupations requiring repetitive overhead work including painters, electricians, construction workers, and warehouse employees face dramatically increased risk from cumulative microtrauma.
Athletes and Overhead Activities
+Athletes performing repetitive overhead motions are highly susceptible. Swimmers, baseball pitchers, tennis players, volleyball players, and weightlifters develop impingement from repetitive stress. Poor technique, inadequate conditioning, and training errors accelerate development.
Anatomic Factors
+Certain anatomic variations predispose to impingement. Hooked or curved acromion shape, os acromiale (unfused acromion), acromioclavicular joint arthritis with inferior spurs, and thickened coracoacromial ligament all narrow the subacromial space increasing compression risk.
Muscle Imbalances and Posture
+Rotator cuff weakness fails to stabilize the humeral head allowing superior migration during elevation. Scapular dyskinesis from weak periscapular muscles causes abnormal mechanics. Poor posture with rounded shoulders and forward head position narrows the space. Previous injuries inadequately rehabilitated create compensatory patterns.
Shoulder Impingement Prevention

Prevention focuses on maintaining optimal shoulder mechanics and avoiding repetitive overhead stress. Strengthen rotator cuff muscles through regular exercises with resistance bands or light weights focusing on external rotation and scapular stabilizers. Maintain proper posture avoiding rounded shoulders and forward head position. Athletes should use proper technique with qualified coaching, adequate rest between training sessions, and gradual progression without sudden volume increases.
Workers performing overhead activities should use proper ergonomics with ladders or scaffolding bringing work to comfortable height, take frequent breaks allowing recovery, and perform stretching exercises throughout the day. Maintain shoulder flexibility through regular stretching of posterior capsule and pectoral muscles. Address early symptoms promptly—persistent pain with overhead activities warrants evaluation before progression to tendon damage. Complete rehabilitation after shoulder injuries before returning to full activities.
How is Shoulder Impingement Diagnosed?
Diagnosis begins with comprehensive history documenting pain location, onset, aggravating activities, and functional limitations. Physical examination includes inspection for muscle atrophy, palpation over rotator cuff and subacromial space, range of motion assessment, strength testing, and special tests. The Neer impingement sign (pain with forced forward elevation) and Hawkins-Kennedy test (pain with internal rotation at 90 degrees flexion) identify impingement. Painful arc between 60-120 degrees is characteristic.
X-rays evaluate bone structure including acromion shape, acromioclavicular joint arthritis, bone spurs, and calcifications. MRI shows rotator cuff integrity, tendon inflammation, bursal thickening, and degree of tendon damage from partial to full-thickness tears. Ultrasound provides dynamic assessment during movement and can visualize tendon pathology. Diagnostic subacromial injection with local anesthetic provides confirmation—significant pain relief indicates impingement as primary pain source. The diagnosis is primarily clinical based on examination findings and symptom pattern.
What treatment is best for Shoulder Impingement?
Treatment approach depends on symptom severity, duration, degree of rotator cuff involvement, and functional goals. Most cases resolve with conservative management over 6-12 weeks. Early intervention prevents progression to irreversible tendon damage. Treatment is individualized based on examination findings and patient response.
Activity Modification and Rest
+Initial treatment includes relative rest avoiding painful overhead activities while maintaining motion through pain-free range. Modify work or sports technique reducing repetitive overhead stress. Ice application after activities reduces inflammation. NSAIDs provide pain relief and decrease inflammation.
Physical Therapy
+Guided physical therapy is cornerstone treatment, focusing on rotator cuff and scapular stabilizer strengthening, posterior capsule stretching, posture correction, and gradual return to overhead activities. Therapists address underlying muscle imbalances and movement dysfunction. Most patients improve significantly with dedicated therapy.
Corticosteroid Injections
+Subacromial corticosteroid injections provide significant pain relief when conservative measures fail, reducing inflammation and allowing participation in physical therapy. Ultrasound guidance ensures accurate placement. Injections combined with therapy show better outcomes than either alone. Limited to 2-3 injections annually to avoid tendon weakening.
Arthroscopic Subacromial Decompression
+Persistent symptoms after 3-6 months of appropriate conservative treatment may warrant surgery. Arthroscopic subacromial decompression removes bone spurs, reshapes the acromion creating more space, removes inflamed bursa, and addresses associated pathology. Minimally invasive approach allows faster recovery. Most patients return to full activities within 3-4 months post-operatively.
Shoulder Impingement Treatment in Cleveland, Ohio

Cleveland Shoulder Institute offers comprehensive impingement treatment using evidence-based protocols. Our multidisciplinary team includes fellowship-trained orthopedic surgeons and specialized physical therapists who collaborate on every case. We utilize advanced diagnostic imaging including MRI and ultrasound to ensure accurate diagnosis and identify contributing factors.
Treatment plans are customized to your specific pathology and goals. Conservative options include targeted physical therapy addressing rotator cuff strengthening and scapular mechanics, activity modification guidance, and ultrasound-guided corticosteroid injections when indicated. For refractory cases, we offer arthroscopic subacromial decompression—a minimally invasive procedure providing excellent relief when conservative treatment plateaus. Post-operative rehabilitation follows structured protocols ensuring optimal recovery. Located in Cleveland with convenient scheduling and comprehensive follow-up.
Schedule Your ConsultationMeet our Shoulder Specialist Team
Our shoulder team consists of fellowship-trained orthopedic surgeons specializing exclusively in shoulder conditions. Each surgeon completed additional advanced training beyond residency, focusing on complex shoulder pathology, arthroscopic techniques, and shoulder reconstruction. They stay current through active research participation, teaching commitments, and regular attendance at specialized shoulder conferences.
Supporting our surgeons are certified shoulder physical therapists, experienced surgical staff, and dedicated medical personnel trained in shoulder-specific protocols. This collaborative approach ensures seamless care from initial evaluation through complete recovery. We believe in conservative treatment when appropriate while offering surgical expertise when needed. Our team takes time to educate patients about their condition, explain all treatment options with realistic expectations, and involve you in decision-making throughout your care.
What Our Patients Say About Our Impingement Treatments
Real results from real patients who regained their shoulder function:
"Six months of shoulder pain as a painter was affecting my work. Physical therapy and an injection got me back to normal within two months. Dr. Martinez really understood my job demands and tailored treatment accordingly."
— Carlos R., Cleveland
"After conservative treatment stalled, the arthroscopic decompression was the right call. Surgery was minimally invasive and recovery was faster than expected. Back to playing tennis pain-free within four months."
— Linda S., Lakewood
"The therapy program was excellent. They addressed my weak rotator cuff and poor posture that were causing the impingement. Pain resolved completely without surgery. Very grateful for their expertise."
— Michael T., Westlake
Shoulder Impingement Frequently Asked Questions
How long does shoulder impingement take to heal?
+Most cases improve with conservative treatment within 6-12 weeks. Mild impingement may resolve in 4-6 weeks with proper rest and therapy. Chronic cases or those with significant rotator cuff involvement may require 3-6 months. Surgery requires 3-4 months for full recovery. Early treatment accelerates healing.
What happens if shoulder impingement is left untreated?
+Untreated impingement progressively damages the rotator cuff. Initially causing inflammation and partial-thickness tears, continued compression leads to full-thickness tears requiring surgical repair. Advanced cases develop irreversible tendon degeneration, muscle atrophy, and arthritis. Early treatment prevents these complications.
Can impingement heal without surgery?
+Yes, most impingement cases heal with conservative treatment including physical therapy, activity modification, and anti-inflammatory strategies. Studies show 70-80% of patients improve without surgery. Surgery is reserved for cases failing appropriate conservative treatment for 3-6 months or those with significant structural abnormalities.
What exercises help shoulder impingement?
+Effective exercises include rotator cuff strengthening with resistance bands focusing on external rotation, scapular stabilizer exercises including rows and wall slides, posterior capsule stretches, and postural exercises. Pendulum exercises maintain motion during acute pain. A physical therapist designs a program specific to your needs.
Is shoulder impingement the same as rotator cuff tear?
+No, but they are related. Impingement is compression of rotator cuff tendons causing inflammation and pain. Untreated impingement can progress to rotator cuff tears. Early impingement shows intact tendons on MRI, while tears show tendon disruption. Treatment differs—impingement often responds to conservative care while complete tears may require surgical repair.