Arthroscopic Biologic Total Shoulder Resurfacing
The arthroscopic biologic total shoulder replacement is a new procedure that I have worked on in partnership with my colleagues at Arthrex, Inc. The procedure is designed to resurface (the orthopedic term commonly referred to as replace) the worn cartilage of the shoulder joint with transplanted donor cartilage and bone. In order to understand the rationale for developing this new procedure, it’s important to consider what is currently done to treat end-stage or late osteoarthritis of the shoulder.
The hallmarks of symptomatic osteoarthritis in the shoulder, as with other joints, are pain and stiffness. Patients who have a painful stiff shoulder usually try conservative treatments in the form of oral anti-inflammatories, activity modification, or physical therapy among other modalities. Once conservative measures to relieve pain and/or increase function have failed, which will typically occur over time as part of the natural history of this disorder, operative intervention may be indicated.
Typical operative treatments employed for arthritis in the shoulder include arthroscopic debridement with or without chondroplasty and capsular release, partial shoulder replacement, or total shoulder replacement. The outcomes for arthroscopic debridement and chondroplasty as well as other experimental procedures are unpredictable according to several studies reported in the literature. The most reliable operative interventions for the treatment of symptomatic late osteoarthritis have been reported with total shoulder replacement or partial shoulder replacements (hemiarthroplasty). These partial or total shoulder replacements involve removing a substantial part of the ball (proximal humerus) and/or socket (glenoid) bone and replacing the bone with metal and/or plastic. There is significant long-term outcomes data for these procedures demonstrating reliable pain relief and improved function for most patients.
The arthroscopic biological total shoulder replacement possesses three potential advantages as a resurfacing procedure over total or partial shoulder replacements with metal and/or plastic parts:
- First, the procedure is done arthroscopically as an outpatient procedure.
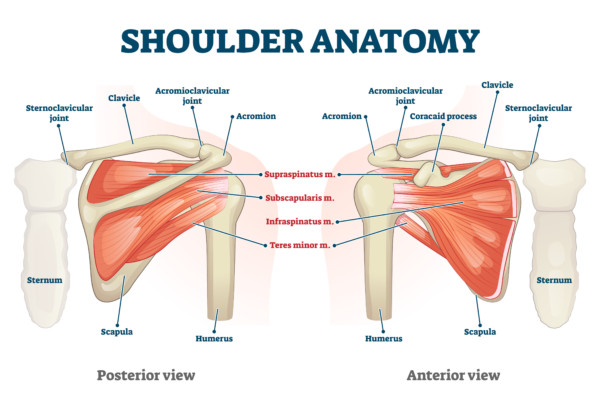
- Second, unlike conventional total or partial shoulder replacement, the arthroscopic total shoulder replacement does not cut through any of the rotator cuff muscles in order to gain access to the shoulder joint in order to perform the replacement. Rather, the arthroscopic technique works between the muscles of the rotator cuff, in a space called the rotator interval, without violating or injuring any of the rotator cuff muscles. Violation of the rotator cuff as part of performing a total shoulder replacement has been reported as a significant source of complications with this procedure.
- Third, one of the primary goals of the arthroscopic biologic shoulder replacement is to replace the worn cartilage of osteoarthritis with transplanted ‘healthy’ cartilage from a cadaver donor rather than synthetic metal and/or plastic as with a conventional partial or total shoulder replacement. Hence, the fact that I am replacing worn cartilage with a biologic material, cadaveric cartilage-bone transplants, is the rationale for the use of the word ‘biologic’ in describing the replacement. The use of cartilage-bone transplants has been employed in numerous orthopaedic procedures with good results in both the shoulder and the knee. The use of cartilage transplantation on the socket (glenoid) of the shoulder is relatively new. However, the use of cartilage-bone cadaver transplants on the ball (humerus) of the shoulder joint has been performed with good results reported. If the arthroscopic biologic total shoulder replacement is able to demonstrate successful durability and wear over time, then I believe it would represent a significant advance in the treatment of osteoarthritis of the shoulder.
Finally, the arthroscopic biologic total shoulder replacement removes a minimal amount of bone that makes revision to conventional total shoulder replacement or arthroscopic revision with another graft technically feasible without ‘burning any bridges.’
The arthroscopic biologic total shoulder replacement is a new procedure and does not have long-term outcomes data demonstrating its efficacy. The main risk for this procedure is that the cartilage-bone transplant may not incorporate, or ‘take’, in a given patient’s shoulder joint. If this problem occurs, a patient who has this procedure may require a second operation, likely a total shoulder replacement with metal and plastic parts, in order to definitely treat the arthritis in the shoulder. I am in the process of organizing a clinical study currently to evaluate this procedure’s efficacy.
In conclusion, the arthroscopic biologic total shoulder replacement is a new and innovative procedure aimed at treating symptomatic late-stage osteoarthritis using cadaver cartilage-bone transplants to replace worn cartilage in the shoulder using an all-arthroscopic outpatient minimally invasive technique that does not violate the rotator cuff. I am performing this procedure on select patients in order to understand whether or not this procedure can successfully treat patients with osteoarthritis of the shoulder by restoring shoulder function and relieving arthritis pain. In my opinion, if this procedure successfully treats osteoarthritis, then it will represent a major advance in the treatment of shoulder arthritis.
Live Surgery Video
– Arthroscopic Biologic Total Shoulder Resurfacing
Open Biologic Total Shoulder Resurfacing
Bulk Head Allograft Resurfacing
Patients who develop global osteoarthritis of the humeral head require larger osteochondral grafts than those that can be inserted arthroscopically through the rotator interval. For these patients, we have developed an open humeral head transplant using a fresh bulk humeral head allograft. This procedure provides younger patients with a solution for severe humeral head osteoarthritis and degeneration that avoids prosthetic implants and minimizes native bone loss. Bulk humeral head allograft transplantation is performed with the patient in the beach-chair position. A standard ‘deltopectoral’ approach to the shoulder is used to provide exposure of the subscapularis muscle and the rotator interval. We find it is easiest to perform a subscapularis tenotomy —cutting of the muscle tendon— to gain access to the glenohumeral joint. The tenotomy must be repaired “end to end” as the humeral canal is not prepared and no prosthesis is implanted to anchor sutures. During the subscapularis tenotomy, we attempt to harvest the entire width of the tendon footprint, that is, from the rotator interval superiorly to the anterior circumflex vessels inferiorly.
The resected native humeral head is then compared with the allograft. The arthritic head is typically flatter and larger in diameter, secondary to degeneration and osteophytosis. Using visual inspection, a humeral neck cut is performed on the allograft that most closely resembles the native anatomy. The harvested allograft is then gently washed and taken back to the surgical field. The humeral head allograft is then placed on the humeral neck cut and “dialed-in” for a best-fit alignment. Once pleased with the position, the graft and humeral neck are marked at the “12-o’clock” position for later reference. With the native humeral head resected, attention is now turned to the condition of the glenoid surface. For patients with isolated humeral head defects without appreciable glenoid arthritis, the glenoid is left alone, and a hemiresurfacing of the humerus is completed. However, if a significant amount of glenoid osteoarthritis is appreciated, our preferred technique is to ream the glenoid to a smooth surface.
Live Surgery Video – Open Biologic Total Shoulder Resurfacing
Published Articles
All-Arthroscopic Biologic Total Shoulder Resurfacing
I am a paid consultant for Arthrex, Inc., and receive monetary compensation related to this procedure.