


Common Labral Repair Symptoms & Causes
Candidates for arthroscopic labral repair experience recurrent shoulder instability or subluxation (feeling of shoulder slipping), history of one or more shoulder dislocations, persistent pain with overhead activities or throwing motions, clicking, popping, or catching sensations with movement, apprehension or fear of shoulder "coming out" during certain positions, weakness with specific movements, and night pain disrupting sleep. Labral tears result from traumatic shoulder dislocations (most common), repetitive overhead activities in throwing athletes or swimmers, direct trauma or falls on outstretched arm, or degenerative changes with aging. Young athletes aged 15-35 with traumatic instability are highest risk group. Each dislocation episode increases labral and capsular damage, making early surgical intervention important to prevent progressive injury and arthritis development.
Schedule Your ConsultationWho's a Candidate for Arthroscopic Labral Repair?
Not everyone with a labral tear requires surgery. Understanding candidacy criteria ensures optimal outcomes and prevents recurrent instability:
Recurrent Instability Episodes
+Ideal candidates have experienced multiple shoulder dislocations or subluxation episodes, or single traumatic dislocation in young active individuals (under 25-30 years old) who face high recurrence risk. After first dislocation, young athletes have 80-90% risk of recurrence without surgery. Multiple dislocations increase bone loss and capsular stretching, making stabilization more critical.
Activity Level and Demands
+Athletes participating in overhead sports (baseball, swimming, volleyball), contact sports (football, hockey, rugby), or activities with fall risk (skiing, mountain biking) are prime candidates. Military personnel and manual laborers with high-demand jobs benefit from surgical stabilization. Sedentary individuals with low activity demands may manage successfully with activity modification and strengthening.
Age and Tissue Quality
+Younger patients (under 40) with good tissue quality achieve best outcomes. First-time dislocations in patients under 25 warrant serious consideration for early surgery due to extremely high recurrence rates. Older patients (over 40) with first-time dislocations have lower recurrence risk and may be managed conservatively unless symptoms persist or activity demands warrant surgery.
Bone Loss and Previous Surgeries
+Significant glenoid or humeral bone loss from recurrent dislocations may require additional procedures beyond simple labral repair—bone grafting or specialized techniques. Failed previous stabilization surgery requires revision with potentially different surgical approach. Realistic expectations and commitment to rehabilitation are essential. Smokers must quit—smoking impairs healing and increases failure rates.
Preparing for Arthroscopic Labral Repair

Proper preparation optimizes surgical outcomes and reduces recurrence risk. Complete pre-operative physical therapy focusing on rotator cuff and scapular strengthening—stronger muscles provide dynamic stability. Stop smoking at least 4 weeks before surgery—smoking significantly impairs labral and capsular healing. Discontinue anti-inflammatory medications as directed. Arrange transportation and assistance for 48 hours post-surgery. Prepare your home with items at accessible heights avoiding overhead reaching initially. Purchase a comfortable immobilization sling—you'll wear this for 4-6 weeks. Fill prescriptions beforehand. Plan time off work—1-2 weeks for desk jobs, 3-4 months for physical labor or overhead work, 4-6 months for return to contact sports. For athletes, coordinate with coaches about season timing—surgery immediately after season allows full recovery before next season. Mental preparation for rehabilitation commitment and gradual return to activities is important—rushing return to sports dramatically increases re-injury risk.
How is Arthroscopic Labral Repair Performed?
The procedure begins with general anesthesia and nerve block for post-operative pain control. You're positioned in beach chair or lateral decubitus position. The surgeon creates 3-4 small arthroscopic portals (5-10mm incisions) strategically placed around the shoulder. An arthroscope is inserted, displaying high-definition images on monitors. Sterile fluid distends the joint for optimal visualization.
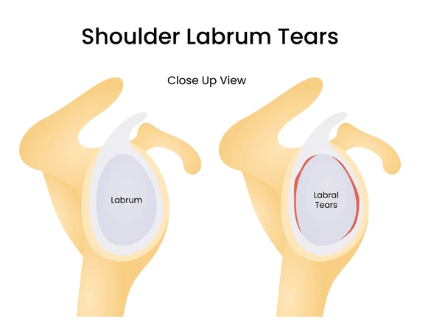
Comprehensive shoulder examination identifies all pathology including labral tear location and pattern, capsular laxity, and associated injuries. The torn labrum is mobilized from scar tissue. The bone surface where labrum should attach (glenoid rim) is prepared by removing soft tissue and creating bleeding bone surface promoting healing. Specialized bone anchors loaded with strong sutures are inserted into the glenoid at strategic locations. Sutures are passed through the labral tissue using various techniques. The labrum is secured back to the bone with appropriate tension, recreating the normal bumper effect. Capsular plication (tightening) is performed to reduce excess capsular volume and enhance stability. The biceps tendon is evaluated and addressed if damaged. Additional pathology like SLAP tears or rotator cuff damage is repaired simultaneously. Portals are closed with sutures. Arm is placed in immobilization sling, often with small pillow positioning shoulder in slight external rotation. Procedure takes 60-120 minutes depending on complexity.
What to Expect After Arthroscopic Labral Repair?
Recovery requires strict compliance with immobilization and rehabilitation protocols. Labral healing takes 12-16 weeks. Premature return to activities dramatically increases re-tear and recurrent instability risk. Athletes require 4-6 months before return to sport. Understanding recovery phases helps set realistic expectations and maximize success.
Immobilization Phase (Weeks 0-4)
+Arm remains in sling continuously for 4-6 weeks protecting labral repair. Some surgeons use abduction pillow positioning shoulder in external rotation, especially for anterior repairs. Nerve block provides 12-24 hours of numbness. Pain medication manages discomfort. Gentle pendulum exercises and elbow/hand motion only. No shoulder motion or muscle activation. Ice reduces swelling. Sleep in recliner or propped up initially for comfort.
Early Motion Phase (Weeks 4-8)
+Sling continues but gentle passive range of motion begins under therapist supervision. Therapist moves arm within safe ranges avoiding positions that stress repair. Gradual progression of motion in protected ranges. No active motion yet. No rotation exercises initially as these stress labral repair most. Driving resumes once off narcotics and with surgeon approval, typically 4-6 weeks.
Active Motion and Strengthening (Weeks 8-16)
+Sling discontinued around 6-8 weeks. Active motion exercises begin. Progressive strengthening starts with isometrics, then resistance bands, then light weights. Focus on rotator cuff and scapular stabilizers. Gradual increase in motion ranges. Light daily activities resume. Most desk work jobs feasible by 8-12 weeks. No sports or heavy activities yet.
Return to Sport Phase (Months 4-6)
+Sport-specific training begins around 4 months once adequate strength and motion restored. Interval throwing programs for overhead athletes. Gradual progression in intensity and volume. Return to contact sports typically 5-6 months. Return to full unrestricted competition 6 months minimum. Some athletes require 9-12 months for complete confidence restoration. Lifetime shoulder maintenance program recommended.
Arthroscopic Labral Repair Surgery in Cleveland, Ohio

Cleveland Shoulder Institute specializes in advanced arthroscopic labral repair and shoulder stabilization procedures. Our surgeons perform over 100 stabilization procedures annually, utilizing the latest anchor technology, suture passing techniques, and capsular management strategies. We have particular expertise treating athletes and high-demand patients requiring reliable stability restoration.
Our comprehensive approach includes thorough pre-operative assessment with advanced imaging (MRI arthrogram when indicated), precise surgical technique tailored to specific tear patterns and bone loss, and sport-specific rehabilitation protocols. We coordinate closely with athletic trainers and physical therapists experienced in return-to-sport progressions. For athletes, we work with coaches to optimize surgical timing around seasons. Surgery is performed at accredited ambulatory surgery centers with high-definition arthroscopic systems. We participate in outcomes research tracking recurrence rates and return-to-sport success. Located in Cleveland with convenient scheduling and expertise managing both primary and revision stabilization procedures.
Schedule Your ConsultationMeet our Shoulder Stabilization Team
Dr. Gobezie is a fellowship-trained shoulder and elbow surgeon who completed advanced training in arthroscopic surgery and sports medicine. He performs hundreds of arthroscopic stabilization procedures annually, maintaining expertise in various labral repair techniques for different tear patterns. Dr. Gobezie has particular experience treating overhead athletes and contact sport athletes requiring reliable stability for safe return to competition. He stays current through active research participation, teaching commitments, and leadership in professional societies.
Supporting Dr. Gobezie are board-certified anesthesiologists experienced in nerve blocks, certified surgical technologists trained in arthroscopic anchor systems, and specialized sports physical therapists with expertise in shoulder stabilization rehabilitation and return-to-sport protocols. Our therapists understand the critical healing phases and progression criteria for athletes. This collaborative approach ensures optimal surgical technique, appropriate repair construct for individual pathology, and safe progressive return to activities minimizing recurrence risk while restoring full function.
What Our Patients Say About Arthroscopic Labral Repair
Real experiences from patients who successfully stabilized their shoulders:
"After three shoulder dislocations playing football, I needed surgery to get back in the game. Dr. Gobezie repaired my labrum arthroscopically. I followed the rehab protocol exactly and returned to football six months later. Two years later my shoulder is rock solid with no instability issues."
— Tyler Jackson
"My shoulder kept subluxing when swimming, limiting my training. The labral repair eliminated the instability completely. Recovery took patience but I'm back swimming competitively with full confidence in my shoulder. The arthroscopic approach meant quick recovery compared to what I expected."
— Amanda Cooper
"I dislocated my shoulder skiing and Dr. Gobezie recommended surgery to prevent future dislocations. The procedure went smoothly and physical therapy was excellent. Five months later I'm back skiing with no apprehension. My shoulder feels stable and strong. Great outcome."
— Brian Mitchell
Arthroscopic Labral Repair Frequently Asked Questions
How long does it take to recover from labral repair surgery?
+Initial healing takes 12-16 weeks with strict immobilization for 4-6 weeks. Return to non-contact activities typically 3-4 months. Return to contact sports and overhead activities 5-6 months minimum. Athletes may require 6-9 months for full confidence restoration and return to competition. Recovery timeline varies by repair complexity and individual healing.
What is the success rate of shoulder labral repair?
+First-time labral repairs have 85-90% success rates in preventing recurrent instability. Success rates are highest in younger patients without significant bone loss. Revision surgeries have lower success rates (70-80%). Compliance with rehabilitation and avoiding premature return to activities significantly impacts success. Most patients achieve excellent stability and return to desired activities.
Can my shoulder dislocate again after labral repair?
+Recurrence risk exists but is significantly reduced compared to non-surgical treatment. Risk is approximately 10-15% after first surgery, higher (20-30%) after revision surgery. Risk factors for recurrence include premature return to sports, significant bone loss, failed repairs, and high-risk contact sports. Following rehabilitation protocols and respecting healing timelines minimizes recurrence risk.
Will I regain full range of motion after surgery?
+Most patients regain functional range of motion, though some may lose 5-10 degrees of external rotation intentionally tightened to enhance stability. This small motion loss rarely affects function and is worthwhile tradeoff for stability. Overhead athletes typically regain full motion needed for their sport with proper rehabilitation. Motion goals are discussed pre-operatively.
When can I return to sports after labral repair?
+Return to sport timing depends on sport demands: non-contact sports 3-4 months, overhead sports 5-6 months, contact sports 6 months minimum. Return criteria include adequate healing time, full pain-free range of motion, 90%+ strength compared to opposite side, and successful completion of sport-specific training. Premature return significantly increases re-injury risk.