Biceps Tenodesis
Surgery for Biceps Tendinosis/Tendinopathy
What is biceps tenodesis?
Biceps tenodesis is a surgery performed to alleviate the pain caused by biceps tendinosis. Arthroscopic surgery is a minimally invasive procedure where surgery is performed via a ‘keyhole’ approach through two or three small incisions using a piece of equipment which is a bit like a thin telescope (an arthroscope).
Do I need to have this bicep surgery?
Biceps Tendonitis will usually resolve within one year. If the pain persists and is generally not relieved with time or cortisone injections, then a patient may consider surgery since it’s likely there are more problems in the shoulder. There is usually no rush on surgery. Until conservative measures are no longer providing a patient with adequate pain relief, particularly if a person is having trouble sleeping, getting dressed, doing their job or preventing them from doing what they want to do, then surgery is usually recommended. This procedure is recommended for patients who have partial or full-thickness biceps tendon tears, biceps instability, SLAP lesions, or biceps tendinopathy. Read more about biceps tendinitis here.
What happens during the bicep tenodesis surgery?
During your surgery you are generally sat up in a beach chair type position. The operation is usually done via keyhole surgery (arthroscopy). The surgeon introduces a camera into your shoulder through a small incision and watches the images on a TV screen. Photos are taken of the findings. Here is the
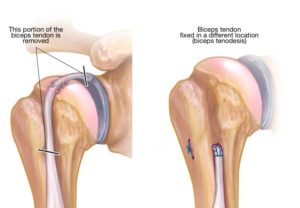
Biceps tenodesis is a procedure during which the surgeon cuts the attachment of the biceps tendon to the labrum (cartilage around shoulder socket) and reattaches it to the humerus (upper arm bone). The benefit of reattaching the tendon below the bicipital groove is restored function and decreased pain. Removing the painful part of the biceps usually resolves symptoms and restores normal function. After the surgery, the small wound is closed using stitches. For more detailed information, you can read Tenodesis: Procedure, Recovery, and Outcomes
Watch: Shoulder Pain When Throwing? Biceps Tendonitis Explained
Understanding the difference between biceps tendon irritation, instability, and tear can help you recognize why you’re feeling pain during rotation or throwing — watch the video below for a clear, expert explanation.
Will I feel any pain in my bicep?
Your arm will feel numb because of the nerve block/local anesthetic used during your operation, but this should wear off during the first 24 hours after the operation. Post-operative pain is normal, and you will receive medication to help minimize this pain.
What are the risks of surgery failure?
As with any surgery, shoulder arthroscopy carries some risk, however, it has been shown to be safe with few complications.
Arthroscopic biceps tenodesis is routinely performed and is generally a very safe procedure. Before suggesting the operation, your doctor will have considered that the benefits of the procedure outweigh any disadvantages. However, to make an informed decision and give your consent, you need to be aware of the possible side effects and complications associated with most surgical operations.
Sugery Complications may include:
- Infection – this is a very serious complication and significant measures are taken to avoid it, for example you will be given antibiotics to try to guard against it.
- Nerve injury – the risk of this is very rare, but if damage occurs further treatment or surgery may be needed.
- Bleeding – this is rarely an issue as arthroscopic capsular release is a ‘keyhole’ procedure with very little blood loss.
- Thrombosis/blood clot – this is rarely an issue in shoulder surgery.
- Symptoms of stiffness may return – this is unusual, but it may become necessary to repeat the operation if the stiffness is troublesome.