

Common Reverse Shoulder Replacement Symptoms & Causes
Candidates for reverse total shoulder replacement experience severe shoulder pain unrelieved by conservative treatments, profound weakness preventing overhead arm elevation, inability to perform basic daily activities like dressing or reaching, nighttime pain disrupting sleep, and significant functional disability. The primary cause is rotator cuff tear arthropathy—a combination of massive irreparable rotator cuff tears with secondary arthritis causing the humeral head to migrate upward. Other indications include failed conventional shoulder replacement, severe fractures with rotator cuff compromise, rheumatoid arthritis with cuff deficiency, and tumor reconstruction. Patients typically have tried physical therapy, injections, and other treatments without adequate relief.
Schedule Your ConsultationWho's a Candidate for Reverse Shoulder Replacement?
Reverse shoulder replacement serves a specific patient population with complex shoulder problems. Understanding candidacy ensures optimal outcomes:
Rotator Cuff Tear Arthropathy
+The primary indication is massive irreparable rotator cuff tears combined with glenohumeral arthritis. Patients experience superior migration of the humeral head, pseudoparalysis (inability to elevate arm), and severe pain. Traditional shoulder replacement fails in this scenario because the rotator cuff cannot stabilize conventional implants.
Age and Activity Level
+Most candidates are over 65-70 years old, though younger patients with massive cuff tears and no other options may be considered. The procedure has activity restrictions—no heavy lifting over 25-30 pounds, no contact sports, no repetitive overhead work. Appropriate candidates understand and accept these permanent limitations.
Failed Previous Surgery
+Patients with failed conventional shoulder replacements, failed rotator cuff repairs with arthritis, or complications from fracture treatment may benefit from revision to reverse replacement. Complex revision cases require specialized expertise and may have modified expectations compared to primary reverse replacement.
Medical Fitness and Deltoid Function
+Candidates must have functioning deltoid muscle—reverse replacement relies entirely on deltoid strength. Previous deltoid injury, nerve damage, or significant deltoid atrophy are contraindications. Active infections, inadequate bone stock, or severe medical conditions preventing surgery disqualify candidates. Realistic expectations and commitment to restrictions are essential.
Preparing for Reverse Shoulder Replacement

Comprehensive preparation optimizes surgical outcomes and implant longevity. Complete all pre-operative medical clearance including cardiac evaluation if indicated. Optimize management of diabetes, blood pressure, and other chronic conditions. Dental examination ensures no active infections that could seed the implant. Stop smoking at least 6-8 weeks before surgery—smoking dramatically increases infection and healing complications. Discontinue blood thinners as directed. Lose weight if overweight to reduce surgical and anesthetic risks. Arrange transportation and full-time assistance for at least one week post-operatively. Prepare your home for one-armed activities and sleeping in a recliner initially. Complete pre-operative physical therapy to maximize remaining function. Mental preparation for significant recovery timeline and permanent activity restrictions is critical for satisfaction.
How is Reverse Shoulder Replacement Performed?
The procedure requires general anesthesia and typically takes 2-3 hours. You're positioned in beach chair position. A deltopectoral incision (4-6 inches) is made over the front of the shoulder. The deltoid muscle is carefully mobilized without detachment. The subscapularis tendon is released to access the joint. The damaged humeral head is removed and the humerus prepared with specialized reamers.
The glenoid (socket) is prepared by removing remaining cartilage and damaged bone. A metal baseplate with central screw and peripheral screws is secured to the glenoid. The glenosphere (ball component) is attached to this baseplate. Attention turns to the humerus where a stem is inserted into the bone canal. The polyethylene socket (cup) component is attached to the humeral stem. The components are reduced (put together) and stability, motion, and tension are assessed. The subscapularis is repaired if tissue quality allows. Incision is closed in layers. Drains may be placed. Arm is placed in immobilization sling. Hospital stay is typically 1-2 nights.
What to Expect After Reverse Shoulder Replacement?
Recovery is lengthy and requires patience. Unlike traditional replacement, reverse replacement relies on scar tissue formation for stability. Protecting the repair and implant during initial healing is critical. Most patients achieve maximum improvement at 12-18 months post-surgery.
Hospital Stay and Early Recovery (Weeks 0-6)
+Hospital stay is 1-2 nights with pain management and early mobilization. Arm remains immobilized in sling for 6 weeks continuously. Passive motion exercises begin immediately but no active motion. Hand, wrist, and elbow exercises prevent stiffness. Ice and pain medication manage discomfort. Wound care and infection monitoring are critical. No driving during this phase.
Active Motion Phase (Weeks 6-12)
+Sling discontinued once healing confirmed. Physical therapy emphasizes active motion exercises gradually restoring shoulder elevation and rotation. Deltoid strengthening is central to functional recovery. Light activities of daily living resume. Driving resumes once off narcotics. No lifting, pushing, or pulling yet.
Strengthening Phase (Months 3-6)
+Progressive strengthening continues with focus on deltoid function and scapular control. Functional activities expand to include most daily tasks. Lifting restrictions begin at 5 pounds, gradually increasing to permanent limit of 25-30 pounds maximum. Most patients achieve plateau of motion by 6 months, though strength continues improving.
Long-Term Recovery (Months 6-18)
+Continued improvement in strength and endurance occurs up to 18 months. Patients reach maximum functional capability with permanent activity modifications. No heavy lifting over 25-30 pounds lifetime. No contact sports, no repetitive overhead work, no high-impact activities. Home exercise program maintains function. Regular follow-up monitors implant integrity and function long-term.
Reverse Shoulder Replacement Surgery in Cleveland, Ohio

Cleveland Shoulder Institute is a regional referral center for complex reverse shoulder replacement procedures. Our surgeons perform over 100 reverse replacements annually, including challenging revision cases and fracture reconstructions. We utilize the latest implant designs with proven track records—lateralized glenospheres, onlay humeral designs, and modular systems allowing customization to individual anatomy.
Our comprehensive approach includes detailed pre-operative planning with advanced imaging and templating, expert surgical technique minimizing complications, multidisciplinary care with specialized orthopedic nurses, and structured rehabilitation programs designed for reverse replacement biomechanics. We participate in national joint registries tracking outcomes. Surgery is performed at hospitals equipped for complex joint replacement with experienced surgical teams. Located in Cleveland, we accept complex referrals from across the region and provide thorough pre-operative consultations ensuring patients understand this life-changing procedure's benefits and limitations.
Schedule Your ConsultationMeet our Reverse Shoulder Replacement Team
Dr. Gobezie is a fellowship-trained shoulder and elbow surgeon who completed advanced training in complex shoulder reconstruction and arthroplasty. He performs high volumes of reverse shoulder replacements annually, including complex primary cases and challenging revisions. Dr. Gobezie stays current through active participation in shoulder arthroplasty research, teaching, and professional societies dedicated to advancing shoulder replacement techniques.
Supporting Dr. Gobezie are orthopedic-specialized anesthesiologists, experienced surgical nurses and technicians trained in joint replacement protocols, specialized physical therapists understanding reverse replacement biomechanics, and case managers coordinating care transitions. Our infection prevention protocols exceed national standards. Social workers assist with discharge planning. This comprehensive team approach ensures optimal surgical outcomes, complication prevention, and coordinated rehabilitation. We provide extensive patient education, realistic expectation setting, and long-term follow-up monitoring implant performance and maintaining function.
What Our Patients Say About Reverse Shoulder Replacement
Real experiences from patients who regained shoulder function through reverse replacement:
""I couldn't lift my arm for two years after my rotator cuff completely tore. Dr. Gobezie said reverse replacement could help when nothing else would. One year later, I can lift my arm overhead and the constant pain is gone. It changed my life.""
— Dorothy Hayes
""The recovery took patience, but it was absolutely worth it. I can now do things I couldn't do for years—reach shelves, wash my hair, get dressed without help. The surgery gave me back my independence. Forever grateful.""
— Frank Sullivan
""After my traditional shoulder replacement failed, I was devastated. Revision to reverse replacement was the answer. The surgical team was excellent and very experienced with complex cases. Two years later, my shoulder functions better than it has in a decade.""
— Barbara Klein
Reverse Shoulder Replacement Frequently Asked Questions
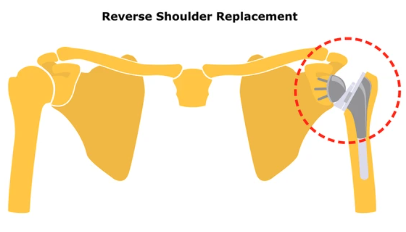
What is the difference between reverse and traditional shoulder replacement?
+Traditional replacement maintains normal anatomy with a ball on the humerus and socket on the glenoid, relying on the rotator cuff for function. Reverse replacement reverses this—ball on glenoid, socket on humerus—allowing the deltoid muscle to compensate for absent or torn rotator cuff. Reverse is used when rotator cuff is irreparably damaged.
How long do reverse shoulder replacements last?
+Modern reverse shoulder implants show excellent survivorship with 90-95% lasting 10+ years and many lasting 15-20 years. Longevity depends on patient age, activity level, bone quality, and adherence to weight restrictions. Younger patients may require revision surgery eventually as implants have finite lifespans.
What are the permanent restrictions after reverse shoulder replacement?
+Permanent restrictions include no lifting over 25-30 pounds repetitively, no contact sports, no high-impact activities, and caution with falls. These restrictions protect the implant and prevent mechanical failure or dislocation. Most daily activities including golf, swimming, and light recreational activities are permitted once fully healed.
What is the success rate of reverse shoulder replacement?
+Success rates exceed 90% for appropriate candidates. Most patients achieve significant pain relief (80-90% reduction), improved function, and ability to elevate arm overhead. Satisfaction rates are high. Complications including infection, nerve injury, dislocation, or mechanical failure occur in 5-10% of cases but are often treatable.
Am I too young for reverse shoulder replacement?
+Age considerations are important as implants have limited lifespans. Most surgeons prefer patients over 65-70 for primary reverse replacement. Younger patients with massive irreparable cuff tears and no other options may be considered, understanding they may need revision surgery in the future and must accept permanent activity restrictions.